December 8, 2024
by Stephen Stofka
This is part 4 of a weekly series of debates on various issues, including climate change, pollution, rent control and market failures in general.
Abel said, “I’d like to pick up where we left off last week, talking about monopolies.”
Cain added, “And monopsonies, you said, where there is only one buyer in a specific market.”
Abel nodded. “There is no better example of both monopoly and monopsony than the health care industry. Your group wants to keep government interference in the market to a minimum. In the health care market, it’s just not possible.”
Cain said, “Private companies offer health insurance. Why do we need government?”
Abel replied, “A product might be labeled health insurance, but insurance companies stay in business by selling risk mitigation. Consumers buy an insurance policy to protect them from a large expense. A for-profit insurance company has an obligation to their shareholders first and they use every legal ruse to reduce the amount they pay on medical claims from their customers.”
Cain argued, “We agree that insurers sometimes deny or delay legitimate claims for care. Congress passed Medicare in 1965 to provide low-cost health care to seniors. The government uses less discretion in paying claims but pays below market rates. That system welcomes fraud and abuse. Health and Human Services estimated that the Medicare and Medicaid programs paid out $100 billion in improper payments in 2023.”
Abel nodded. “The price system doesn’t account for dishonesty by private providers. All the more reason why there has to be greater supervision by government agencies to ensure compliance. A frequent police presence incentivizes people to police themselves.”
Cain disagreed, “No, the government has become a monopsony in the healthcare market. Providers are attracted to Medicare because there is such a large pool of buying power. Providers and suppliers are eager – too – eager – to diagnose and treat older people. Those are resources that cannot be spent on younger people.”
Abel countered, “Younger adults in their prime working years use far less health care services than older people. Without government subsidies, an insurance company would need to charge a prohibitively high rate to insure 70-year-olds.”
Cain asserted, “When people or things get old, they require more service. Imagine if the government funded low-cost auto repairs on cars that were more than ten years old. Car makers would be reluctant to develop improvements in newer car models. Why bother? There is more profit in fixing up the old cars.”
Abel protested, “That’s a stupid analogy. People are not cars.”
Cain nodded. “Exactly. My point is that our society is currently spending a lot of money on old people and the diseases that affect old people. That money is not available to help young people, the newer models of people.”
Abel argued, “Your group sees every problem in dollars and cents. Health care is about human dignity and flourishing as well as the alleviation of suffering, especially for older people who have spent a lifetime working and contributing to their community. What is the price of human dignity? The price system is incapable of measuring the value of intangibles that are precious to us. Government’s role is to protect those qualities we hold dear and that takes regular intervention. Government can’t just step in, assign property rights and let the private market and the price system manage the problem.”
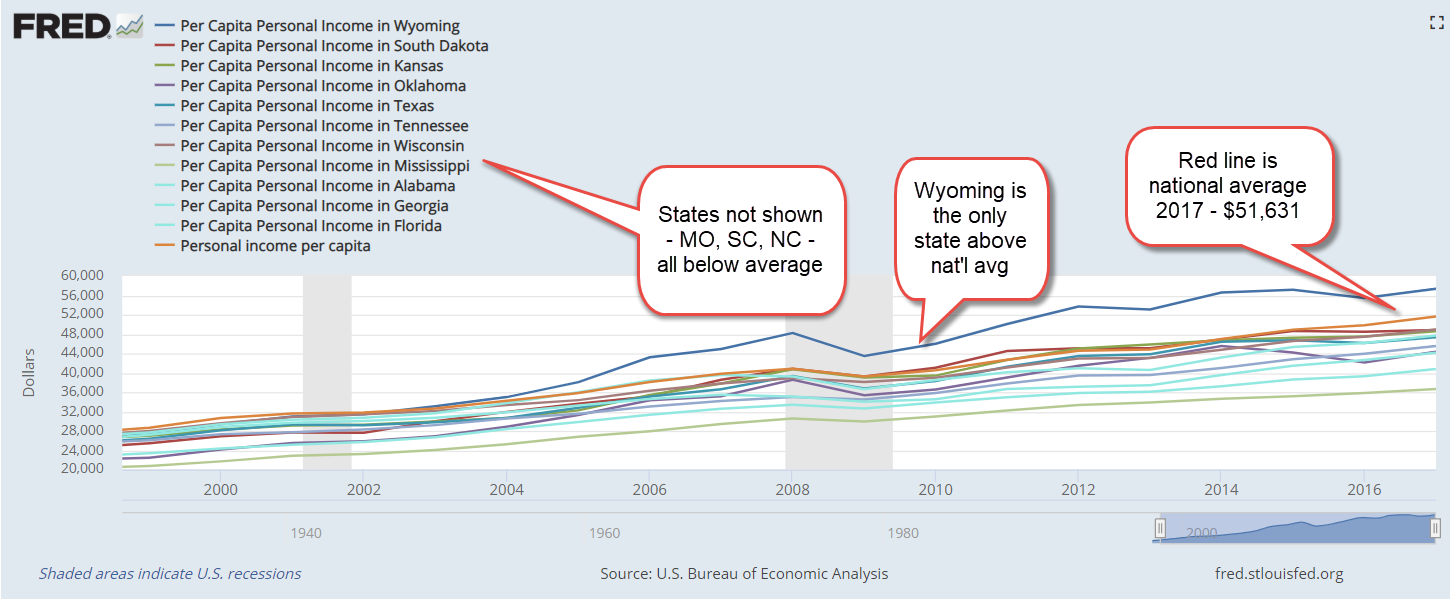
Cain shook his head. “As a share of GDP, healthcare spending in this country continues to grow larger. Per capita spending on healthcare has more than doubled since 2001. The Centers for Medicare and Medicaid Services says that the share was 17.3% in 2022. Out of every $6 of economic activity in this country, more than $1 is spent on healthcare.”
Abel explained, “But that’s because the Boomer generation is so large, and many are seniors. Naturally, healthcare spending will rise because older people use more healthcare services.”
Cain replied, “Yeah, but Medicare spending as a share of total healthcare costs was rising before any of the Boomers became eligible for Medicare. In 2001, Medicare spending was just $1 out of every $5 spent on healthcare. By 2011, that share was more than $1 out of every $4 and the first Boomers had just turned 65 and become eligible for Medicare. In 2021, Medicare spending accounted for almost $1 out of every $3 spent on healthcare (FRED chart and data here). Out of $20 spent in the entire economy, the government now spends $1 taking care of old people. And that doesn’t include Medicaid spending on low- income seniors. That is a burden on younger generations.”
Abel said, “Those costs went up in the 2000s after Republicans revised the Medicare Advantage, Part C, program and added a drug benefit, Part D. Obamacare expanded the program even further. The latest annual report to Congress from the Medicare Payment Advisory Commission found that Medicare Advantage plans paid providers 122% of the amount paid for similar services to Fee-For-Service plans under traditional Medicare.”
Cain replied, “That illustrates my point. When politicians and government agencies try to improve any program, they don’t make the program more efficient. They spend more money. The people who work in government want to codify their principles, their ideals, their sense of fairness into law. Despite their rhetoric, they do not serve the cause of efficiency. They only make things more expensive and more complicated for the people they are supposed to serve.”
Abel countered, “I’ll repeat, your group looks only at the dollars and cents. In 1965, a 65-year-old male could expect to live another 13 years. In 2021, that same male could expect to live another 17 years. Women have had a similar increase of almost four years in life expectancy. The government is spending more on seniors because they are living longer and living better, thanks to the Medicare program. A 70-year-old Boomer today is far healthier and more active than a 70-year-old was in 1965. The price system can not value improvements in the quality or quantity of life.”
Cain argued, “When the government buys almost a third of the entire healthcare market, that’s effectively a monopsony, which distorts the price system. With a functioning market, seniors would pay more for those healthcare services which improved their quality of life. Instead, the government writes the checks, so seniors overconsume healthcare services. Why not? It’s effectively free. That distorts any measure of value that the price system can determine.”
Abel shook his head. “Seniors on fixed incomes have reduced options. There is too much danger that they will forego needed medical care simply because they can’t afford it. For most of their lifetime, they got over respiratory diseases like colds. After an initial visit, injuries like broken bones healed. It may be difficult for seniors to understand that the diseases of old age will not just go away on their own. High blood pressure and heart disease, Type 2 diabetes, arthritis and chronic respiratory problems need active management. Putting off care for a lack of funds only makes those conditions less manageable.”
Cain said, “Educating seniors is the key. Instead, the government treats old people like children. The Medicare program lacks the discipline that private insurance companies bring to the market.”
Abel objected, “A doctor specializing in breast cancer shouldn’t have to justify his recommended course of treatment to some clerk at an insurance company. That’s not a disciplined approach. That’s abuse by an insurance company and people die from that abuse.”
Cain said, “Some unfortunate cases get all the headlines. The government pays out $100 billion in improper payments. That is taxpayer abuse but there is no identifiable victim so that news story runs on page 6. Everyone is so accustomed to government inefficiency and abuse that another example of it causes little outcry. Politicians depend on a voting public that has become numb to the ineptness and unfairness of the political process. Congress has an approval rating of less than 20% but every two years, over 90% of House members are re-elected. Voters act like they are wind up toys.
Abel sighed. “Your group has a deep skepticism of government. Is that likely to change? Probably not. What’s the point of debating these issues if you have a fundamental distrust of government?”
Cain replied, “Hope. Hope that together we can struggle toward some compromise that can curb the excesses of elected and unelected officials.”
Abel nodded. “Ok, we’ll try again next week. Try to think of a public goods program you like. I can see that Medicare is not one of them.”
Cain replied, “See you then.”
///////////////
Photo by Dominik Lange on Unsplash
Medicare Spending charted by Federal Reserve https://fred.stlouisfed.org/series/W824RC1
Per capita healthcare spending, FRED Series https://fred.stlouisfed.org/series/HLTHSCPCHCS
Medicare spending as a share of total health expenditures https://fred.stlouisfed.org/graph/?g=1BYRn
Period Life Expectancy 2004 – 2021 from the Social Security Administration https://www.ssa.gov/oact/STATS/table4c6.html
Period Life Expectancy 1940 – 2001 from the Social Security Administration https://www.ssa.gov/OACT/TR/TR02/lr5A3-h.html
Series of Gallup surveys rating Congress https://news.gallup.com/poll/1600/congress-public.aspx
Re-election rates for House members https://www.opensecrets.org/elections-overview/reelection-rates
A Kaiser Family Foundation brief on the annual report from the Medicare Payment Advisory Commission https://www.kff.org/medicare/issue-brief/medicare-advantage-in-2024-enrollment-update-and-key-trends/
A report on improper Medicare and Medicaid payments https://www.justice.gov/archives/jm/criminal-resource-manual-976-health-care-fraud-generally
//////////////////